INDT-ADHD Module for
Attention Deficit Hyperactivity Disorder
Objectives of The Module
- Overview on Attention-deficit/hyperactivity disorder (ADHD)
- Describe the clinical features/ Core symptoms of ADHD
- Description of INDT-ADHD tool
- Clinically evaluate a child with ADHD using DSM-IV TR criteria using INDT-ADHD tool
- Changes in DSM 5: Need for Modification of INDT-ADHD Tool
ADHD: Definition
- DSM-IV: ADHD is a behavioral and neurocognitive condition characterized by developmentally inappropriate and impairing levels of gross motor overactivity, inattention, and impulsivity"
DSM-IV Criteria for ADHD
- An onset before 7 years of age
- Duration of symptoms greater than 6 months
- An 18 item symptom list of which 6 of 9 inattention or 6 of 9 hyperactive/impulsive symptoms for at least 6 months to a degree that is maladaptive and inconsistent with developmental level
- Some impairment in two or more settings
- Symptoms that do not occur exclusively during the course of pervasive developmental disorder, schizophrenia, or other psychotic disorder that are not better accounted for by another mental disorder, such as depression
DSM-IV Criteria
Inattentiveness
- Is forgetful in daily activities
- Has difficulty sustaining attention
- Has difficulty organizing tasks
- Often loses items necessary for completing a task
- Fails to give attention to detail; makes careless mistakes
- Avoids tasks requiring mental effort
- Easily distracted by extraneous tasks
- Doesn't follow through/fails to finish projects
- Doesn't seem to listen when spoken directly
DSM-IV Criteria
Hyperactive symptoms
- Talks excessively
- Fidgets or squirms excessively
- Leaves seat when inappropriate
- Runs about/climbs extensively when inappropriate
- Has difficulty playing quietly
- Often "on the go" or "driven by a motor"
DSM-IV Criteria
Impulsive symptoms
- Interrupts or intrudes on others
- Cannot await turn
- Blurts out answers before question is finished

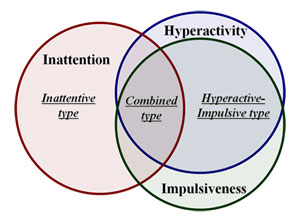
ADHD: Subtypes
Subtypes
- Predominantly Inattentive Type
- Predominantly Hyperactive-Impulsive Type
- Combined Type
Clinical Features: Hyperactivity

- Always moving
- Being on the go
- Changes the focus of activity frequently
- Appears to be without purpose or goal
- Marked clumsiness, accident prone
Example: Frequently leaves table during meal, can't sit still while listening to a story, in continuous state of motion even when watching television.
Clinical Feature: Impulsivity
- Shifts activities unpredictably
- Behavior may be disruptive and dangerous even without provocation
- Often blurts out answers before hearing the whole question
- Does not listen to parents
- Does not learn from mistakes
- Unresponsive to praise or punishment

Clinical Feature: Inattention
- Easily distractible
- Does not complete activities
- Cannot play alone
- Very disorganized
- Cannot deal with complex stimuli in a planned way

Example: Child cannot concentrate on a single activity for more than a few minutes and shifts to another activity frequently.
Consensus Clinical Criteria (CCC)
- The criteria for diagnosis is based on best currently available evidence and / or consensus among national and international experts, using minimal investigations to serve the needs of resource-constrained settings
- Questionnaires and direct observation (both structured and unstructured settings)
- Based on DSM-IV TR criteria
Diagnostic Criteria Consensus Clinical Criteria
Inattention
- Six or more of the following symptoms of inattention have persisted for at least six months to a degree that is inconsistent with developmental level and maladaptive
* Diagnostic & Statistical Manual of Mental Disorders Fourth Edition- Text Revision (DSM IV-TR)
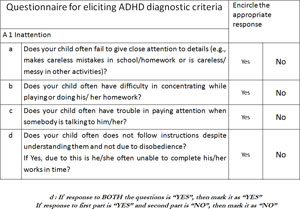
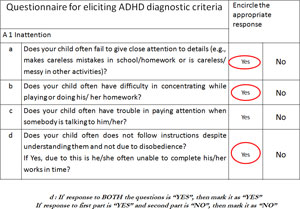
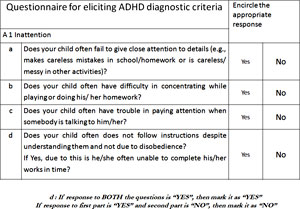
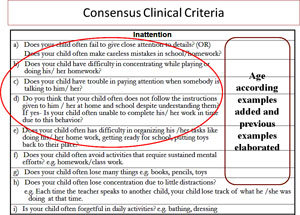
Consensus Clinical Criteria for Inattention
Inattention
- Does your child often fail to give close attention to details? (OR)
- Does your child often make careless mistakes in school/homework?
- Does your child have difficulty in concentrating while playing or doing his/ her homework?
- Does your child have trouble in paying attention when somebody is talking to him/ her?
- Do you think that your child often does not follow the instructions given to him / her at home and school despite understanding them? If yes- Is your child often unable to complete his/ her work in time due to this behavior?
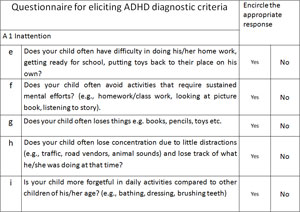
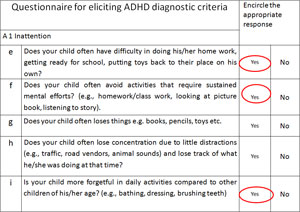
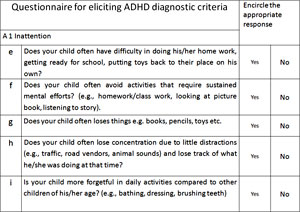
- Does your child often has difficulty in organizing his /her tasks like doing his/ her home work, getting ready for school, putting toys back to their place?
- Does your child often avoid activities that require sustained mental efforts? e.g. homework/class work.
- Does your child often lose many things e.g. books, pencils, toys
- Does your child often lose concentration due to little distractions?
e.g. Each time the teacher speaks to another child, your child lose track of what he /she was doing at that time.
- Is your child often forgetful in daily activities? e.g. bathing, dressing
Diagnostic Criteria Consensus Clinical Criteria
Hyperactivity-impulsivity
- Six or more of the following symptoms of hyperactivity-impulsivity have persisted for at least six months to a degree that is inconsistent with developmental level and maladaptive
* Diagnostic & Statistical Manual of Mental Disorders Fourth Edition- Text Revision (DSM IV-TR)
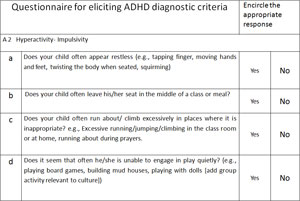
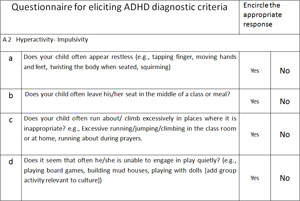
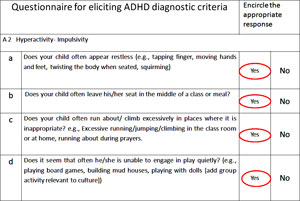
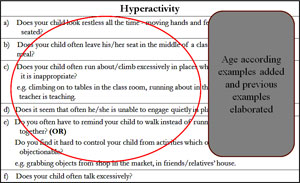
Consensus Clinical Criteria for Hyperactivity
Hyperactivity
- Does your child look restless all the time - moving hands and feet / twisting the body when seated?
- Does your child often leave his/her seat in the middle of a class or meal?
- Does your child often run about/climb excessively in places where it is inappropriate?
e.g. climbing on to tables in the class room, running about in the classroom while the teacher is teaching.
- Does it seem that often he/she is unable to engage quietly in play?
- Do you often have to remind your child to walk instead of running when you are out together? (OR)
Do you find it hard to control your child from activities which others may find objectionable?
e.g. grabbing objects from shop in the market, in friends/relatives' house.
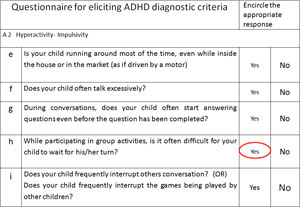
- Does your child often talk excessively?
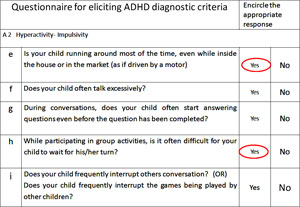
Consensus Clinical Criteria for Impulsivity
Impulsivity
- During conversations, does your child often start answering questions even before the question has been fully asked?
- While participating in group activities, is it often difficult for your child to wait for his/her turn?
- Does your child frequently interrupt others conversation?
(OR)
Does your child frequently interrupt the games being played by other children?
ADHD - Diagnostic Criteria Consensus Clinical Criteria
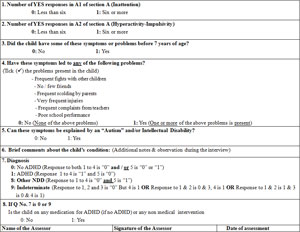
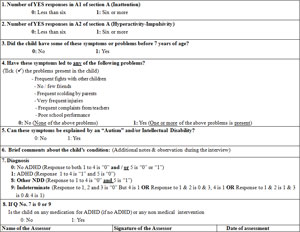
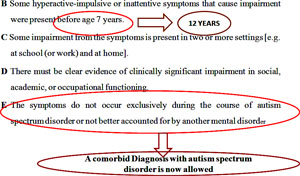
B Some hyperactive-impulsive or inattentive symptoms that cause impairment were present before age 7 years.
C Some impairment from the symptoms is present in two or more settings [e.g. at school (or work) and at home].
D There must be clear evidence of clinically significant impairment in social, academic, or occupational functioning.
E The symptoms do not occur exclusively during the course of autism spectrum disorder or not better accounted for by another mental disorder
Diagnostic Criteria Consensus Clinical Criteria
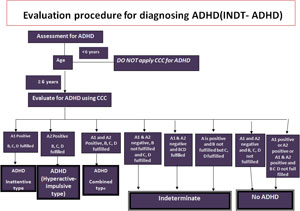
- Diagnosis of ADHD can not reliably be made in children younger than 6 years of age. Hence the consensus clinical criteria should be applied only to children aged 6 years and above
- All the criteria i.e A1 / A2, B, C and D must be fulfilled to make a diagnosis of ADHD according to CCC
ADHD: Comorbidities
- Specific learning disability
- Oppositional Defiant Behavior (negativistic, defiant, disobedient, and hostile behavior toward authority figures)
- Conduct Disorder
- Anxiety and depression
- Epilepsy
- Tourette Syndrome (disorder of recurrent, multiple motor and vocal tics with onset before the age of 18 years)
Differential Diagnosis
- Vision/hearing impairment
- Conduct disorder and oppositional defiant disorder
- Learning disorder
- Epilepsy
- Psychosocial stress
- Drugs side effect
- Inappropriate school or home environment
Heidi et al ;ADHD in children and adoloscentsN Engl J Med 2014;370:838- 46
ADHD: Epidemiological Burden
- Most prevalent neurodevelopmental disorder among children[1]
- In the United States, approximately 5.4 million children between 6 and 17 years of age (9.5% of all U.S. children) have received an ADHD diagnosis[2]
- The prevalence of this condition increased by 33% between 1997–1999 and 2006–2008
[1][2]Poster et al Diagnosed attentionDef icit hyperactivity disorder and learning disability: United States, 20042006. Vital Health Stat 10 2008;237:1-14.
Boyle CA, Boulet S, Schieve LA, et al. Trends in the prevalence of developmental Disabilities In US children, 1997-2008. Pediatrics 2011;127:1034-42
Epidemiological Burden: ADHD
- ADHD has 3-5% prevalence in school aged children worldwide [1,2]
- In the West, studies have shown that ADHD can be reliably diagnosed across clinicians [3]
- This may not be true in India and other similar settings due to low levels of awareness and expertise about ADHD in community clinicians
INDT-ADHD Indian prevalence
- Rural: 1.25%
- Urban :1.64%
- Overall:1.33%
[1] polanczyk G et al, The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry2007 Jun;164(6):942-8
[2] srinath S et al ; Epidemiological study of child & adolescent psychiatric disorders in urban & rural areas of Bangalore, India. Indian J Med Res. 2005 Jul;122(1):67-79
[3] Diagnosis and treatment of attention-deficit/hyperactivity disorder (ADHD). J Am Acad Child Adolesc Psychiatry. 2000; 39:182-93
Epidemiological Burden: ADHD
- Boys more affected than girls [1]
- In a UK survey of 10,438 children aged five to 15 years, Ford 2003 found that 3.62%of boys and 0.85%of girls had a diagnosis of ADHD
- The Center for Disease Control and Prevention in the USA conducted a survey of 102,353 parents with children aged four to 17 years and found a lifetime childhood diagnosis of 7.8%(2.5 times as many boys as girls)
[1]cochrane review 2011:Parent training interventions for Attention Deficit Hyperactivity Disorder (ADHD) in children aged 5 to 18 years
ADHD: Implications; Need for Early Diagnosis
- Compared with their peers, children with ADHD do less well in school[1] and in the development of social skills[2]
- Inattention stops them from focusing on a single task for any length of time
- Their impulsivity disrupts schoolwork
- Their hyperactivity makes them fidget and talk excessively
- The impairments associated with ADHD continue into adolescence
[1] Barkley, R. A. (1997a). Inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD.Psychological Bulletin, 121, 65–94.
[2]Rucklidge JJ, Tannock R. (2001). Psychiatric, psychosocial, and cognitive functioning of female adolescents with ADHD. Journal of the American Academy of Child and Adolescent Psychiatry 40(5):530-540.
ADHD: Need for Early Diagnosis
- Adolescents with ADHD have high rates of delinquency[1] and are more likely to be arrested than non-ADHD teenagers [2]
- They are also at high risk for substance use disorders
- The impulsivity and hyperactivity of ADHD puts individuals at Risk of injury, as has been demonstrated in an analysis of the Pediatric trauma registry of injury managed by 70 hospitals in the USA[3]
- Children with ADHD were more likely to sustain severe injuries than those without ADHD
[1] Barkley, R. A. (1997b). ADHD and the nature of self control. New York: Guilford Press
[2](Satterfield et al. Prediction of antisocial behavior in attention-deficit hyperactivity disorder boys from aggression/defiance scores.J Am Acad Child Adolesc Psychiatry. 1994 Feb;33(2):185-90
[3] DiScala et al. 1998 Injuries to children with attention deficit hyperactivity disorder. pediatrics1998 Dec;102(6):1415-21
ADHD: Early Pointers
- Motor Restlessness
- Difficulty in toilet training
- Destructive play
- Argumentative and excessive temper tantrums
- Excessive demand for parents'/teachers' attention
- Seem to hate waiting and get bored easily
Need for Indigenous Tool
- Appropriateness of construct of the DSM-IV diagnostic criteria had not been studied in the Indian cultural context
- Uses of narrow band rating scales are limited by bias, cost, extensive training requirement, decreased availability and poor applicability
- Some tools require the teacher's perspective of the child's behavior which may not be as reliable given the high student-teacher ratios in Indian settings
Instruction of INDT-ADHD Tool
Instructions for administration:
- Primary caregiver must be present during the assessment for history along with child
- The informant should have been staying with the child for at least 6 months
Instructions for Administration
- The behavior in question
- should be present currently and a usual feature
- should have been present for the last 6 months
- Explain to the parents that the behaviors should be compared with children of same age and background
- Ask the questions verbatim
- Question can be repeated if the respondent cannot understand. Still, if the respondent cannot understand, examples for the particular behavior may be provided which are appropriate to the child's background (rural/ urban, school going/ not school going)
- No further elaboration is allowed

Case Vignette 1
- A 9 year boy has been referred to a child Psychiatrist at the request of his school teacher, because of the difficulties he creates in class.
- His teacher complains that:
- He is so restless that the rest of the class is unable to concentrate
- He is hardly ever in his seat and roams around in the class
- Talks to other children while they are working
- He seems to have no control over his behavior which is unpredictable and can even be quite outrageous
Complaints
- His mother says that his behavior has been difficult since he was a toddler
- Even when he was around 4-years old he was unbearably restless, demanding and forgetful about his daily activities
- He required little sleep and awoke before anyone else
- When he was five, he had managed to unlock the door of the house and wander off into a busy main street
- Fortunately, he was rescued from the oncoming traffic by a passerby
- He was asked to leave a play school because of his difficulty in following instructions and paying attention in class
Complaints
- Presently he avoids doing his home work
- He has minimal interest in TV (only a few selected programs), and dislikes games or toys that require prolonged concentration or patience.
- At home he prefers to be outdoors. However, he is not popular with other children because he cannot await his turn and picks up fights easily.
- Whenever he plays with toys, his games are messy and destructive, and his mother cannot get him to keep his things away tidily.
What symptoms of ADHD does this boy have? List out his symptoms of inattention, hyperactivity & impulsivity separately?
Does he fits into the diagnosis of
ADHD according to you?
- Only inattention.
- His behavior typically demonstrates the characteristic inattention symptoms of ADHD (A1-a, b, d, e, f, i)
Case Vignette 2
- An 8 year old boy was brought to the OPD with complaints of pharyngitis
- Through the open door, the physician noted that the child was pushing others, running about and jumping from one bench to the other when he was waiting outside. His mother was having trouble trying to restrain him
- However, on entering the doctor's room, he was an alert, quiet child who however kept on getting distracted by noises outside
Complaints
- On inquiry, the parents said that the child has been like this since 6 years of age and frequently engages in dangerous activities like jumping from walls, running on the road and breaking household objects
- His teachers also frequently complain that his behavior disturbs others in the classroom during classes
- He often leaves the seat in class and when seated fidgets with hands or feet
- Nobody wants to sit next to him
- Even while playing in school he cannot remain engaged in one game for more than ten minutes
- While playing cricket he can not wait for his turn for batting.
Answer
- He fulfills the following criteria A2- a, b, c, d, e (Hyperactivity) and h
- (Impulsivity)
- These symptoms have been persisting for about one year and affecting his school performance
- Onset of symptoms was around 6 years of age
- Hence, a diagnosis of ADHD can be made using CCC
Case 3
- A six year old boy, was admitted in school 4 months back. He was brought to the psychologist by his mother along with his school teacher
- She was concerned that, he has difficulty in concentrating in the class and got easily distracted
- She had been noticing these behaviours during past three months. She also felt that he talks too much and often made careless mistakes in his home work book
- His mother complained that he often lost pencils and note books in school
- However she said that he could organize his activities like preparing his school bag and keeping his toys in their place
- He could also get ready for school on his own including tying shoe laces and buttoning
Can we make a diagnosis of ADHD based on CCC?
- No; although child has some symptoms of inattention and hyperactivity, he does not have ADHD.
- Reasons are: these symptoms are mainly present in school environment.
- He has no problems at home. Moreover, he has these symptoms for past three months only.
- Hence, at this point of time, he does not fulfill the CCC for diagnosis of ADHD
DSM-IV to DSM -5: Changing Paradigm
- Subtypes are unstable over time
- Some critics view inattention (I) and hyperactivity-impulsivity (HI) as separate elements within a complex disorder.
- The structure of the subtypes (that include a mixture of both HI and I) does not reflect that.
- Other thoughts: I and HI as arbitrarily divided elements of a continuous-trait dimension The current subtype structure offends both schools of criticism
DSM-IV to DSM -5: Changing Paradigm
- Predominantly inattentive ADHD is one of the most frequently used diagnoses in very large samples of treated children.
- Many of these children show few, if any, manifestations of hyperactivity. However, the current subtype structure does not accurately allow for purely inattentive children
- The existence of subtype entities lends weight to their being real, although evidence to support their differentiation in nature (as defined in the DSM-IV) is limited
DSM-IV to DSM -5: Changing Paradigm
- The representation of hyperactivity, inattention, and impulsivity in the criterion set is uneven and, thus, differentially weights some features over others. Impulsivity is underrepresented, and inattention is overrepresented
- Subtype organization leads to threshold artifacts, e.g., ten criteria may be present (five in inattention and five in hyperactivity), and the child would not be eligible for a diagnosis
Comparison Of DSM-IV & DSM-5
Similarities:
- The same 18 symptoms are used as in DSM-IV, and continue to be divided into two symptom domains (inattention and hyperactivity/impulsivity)
- At least six symptoms in one domain are required for diagnosis out of nine
Comparison Of DSM-IV & DSM-5
Changes:
- Examples have been added to the criterion items to facilitate application across the life span
- The cross-situational requirement has been strengthened to "several" symptoms in each setting
- The onset criterion has been changed from "symptoms that caused impairment were present before age 7 years" To "several inattentive or hyperactive-impulsive symptoms were present prior to age 12
Comparison Of DSM-IV & DSM-5
Changes :
- Subtypes have been replaced with presentation specifiers that map directly to the prior subtypes
- A comorbid diagnosis with autism spectrum disorder is now allowed
- A symptom threshold change has been made for adults, to reflect their substantial evidence of clinically significant ADHD impairment, with the cutoff for ADHD of five symptoms, instead of six required for younger persons, both for inattention and for hyperactivity and impulsivity.

INDT-ADHD Tool
- The INDT-ADHD diagnostic tool for ADHD is a freely available tool, developed for the resource limited settings through expert consensus based on established DSM-IV-TR criteria.
- Suitable for Indian cultural context
- Easily administered
- Can be administered by community health workers after a brief training session
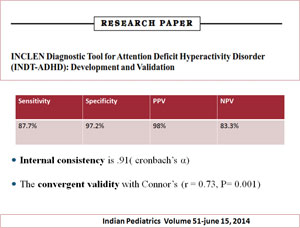
INDT ADHD Tool: Merits
- High diagnostic accuracy
- Adequate content validity
- Good internal consistency
- High criterion validity
- Moderate convergent validity
- Easy to administer
- Free of cost
INDT ADHD Tool: Need for Modification
- Gold standard for diagnosis now is DSM-5 and this tool was based on previous Gold Standard i.e DSM-IV
- Lack of scoring system
- Expanded age group
Modified INDT Tool for ADHD
- Developing a modified INDT-ADHD tool based on DSM-5
- Validation of modified INDT-ADHD Tool based on DSM-5
- Develop a scoring system for follow up of ADHD patients
Changes :Consensus Clinical Criteria (CCC)
- The criteria for diagnosis is based on best currently available evidence and / or consensus among national and international experts, using minimal investigations to serve the needs of resource-constrained settings
- Questionnaires and direct observation (both structured and unstructured settings)

Diagnostic Criteria Consensus Clinical Criteria*
Inattention
- Six or more of the following symptoms of inattention have persisted for at least six months to a degree that is inconsistent with developmental level and maladaptive

Diagnostic Criteria Consensus Clinical Criteria*
Hyperactivity-Impulsivity
Six or more of the following symptoms of hyperactivity-impulsivity have persisted for at least six months to a degree that is inconsistent with developmental level and maladaptive.
Consensus Clinical Criteria
ADHD - Diagnostic Criteria
Consensus Clinical Criteria
Diagnostic criteria�Consensus Clinical Criteria
- Diagnosis of ADHD can not reliably be made in children younger than 6 years of age. Hence the consensus clinical criteria should be applied only to children aged 6 years and above
- All the criteria i.e A1 / A2, B, C and D must be fulfilled to make a diagnosis of ADHD according to CCC
Summary
- Attention deficit hyperactivity disorder is a common neuro-developmental disorder
- Early diagnosis and early initiation of behavioral therapy could be useful
- INDT-ADHD is a good Indian tool for diagnosis of ADHD
- Need for further research and development of Indian tool based on DSM-5
