Outline of Presentation
- Prologue
- Goals of treatment
- Therapies: evidence
- Medical management
- Anecdotal treatment
- Complimentary and Alternative Medicine
- Summary
Prologue
- ASDs are not “curable,” hence chronic management across life span is necessary
- Variable outcomes & dynamic behavioral characteristics
- Most children with ASDs remain within spectrum as adults
- Need constant support with independent living, employment & social relationships
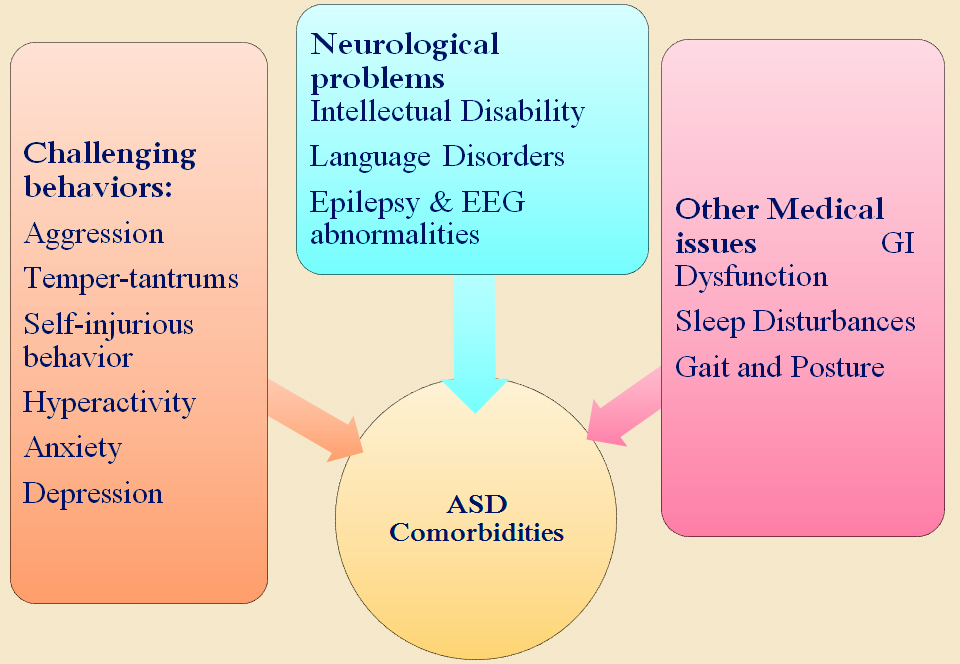
Intervention Targets
- Core features: Social interaction, Communication & Stereotypy
- Non-core features or challenging behaviors: Irritability, Aggression, Hyperactivity, Insomnia, Self-injury
- Co morbid states: such as OCD, depression and anxiety, GI disturbances, epilepsy etc
- Activities of daily living
- Quality of life: individual and family
- Facilitating development and learning, promoting socialization, reducing maladaptive behaviors,
- Without causing adverse effect
ASD: Management
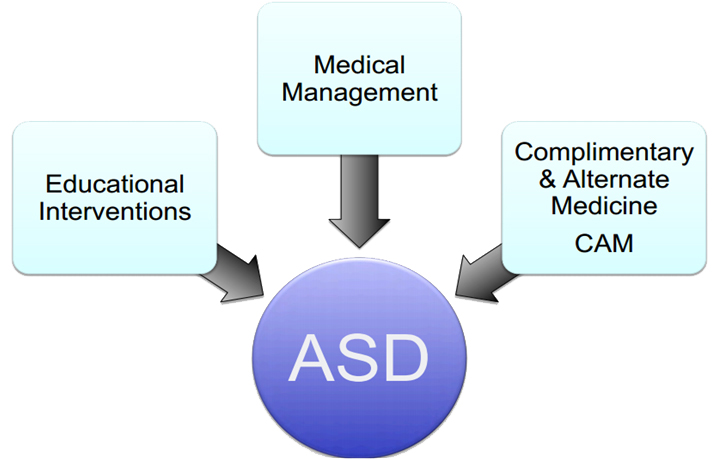
Educational Interventions / Behavioral�Strategies / Rehabilitative Therapies
Different guiding principles
- Academic learning, socialization-communication, managing extreme behaviors, daily-living skills, play and leisure skills
- Involvement of therapist, parents and school teachers
- Frequency, intensity ?
- Does one type fits everybody ? Combinations & ideal prescription ?
- Complete psychological assessment: IQ / Behavior mapping / Sensory issues / co-morbidities / RRB
- Involvement of family, availability, affordability ?
Pick & Choose
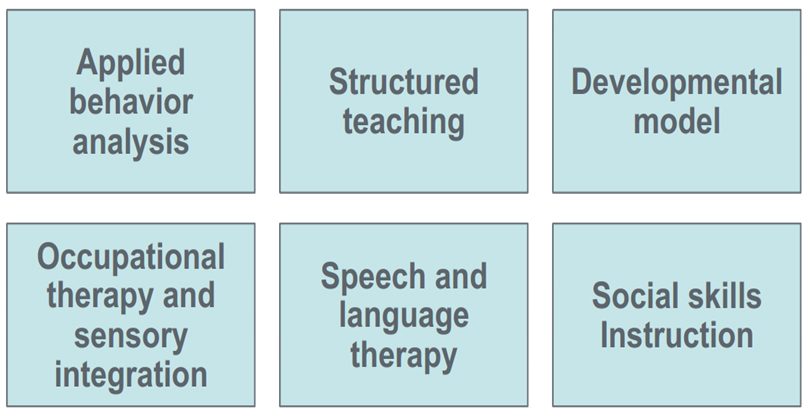
Educational Interventions & Principles
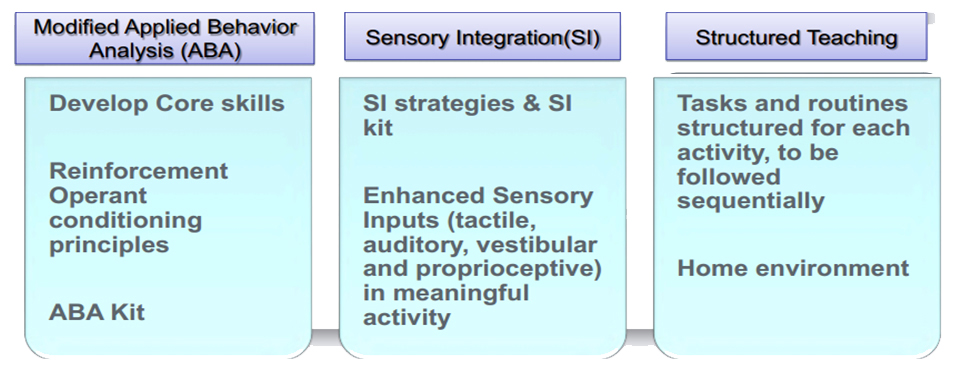
Applied Behavior Analysis
- Interventions that are based on principles of learning derived from research to systematically change behavior
- Early intensive behavioral treatment: substantial, sustained gains in cognitive ability, language, and adaptive behavior
- Also some measures of social behavior
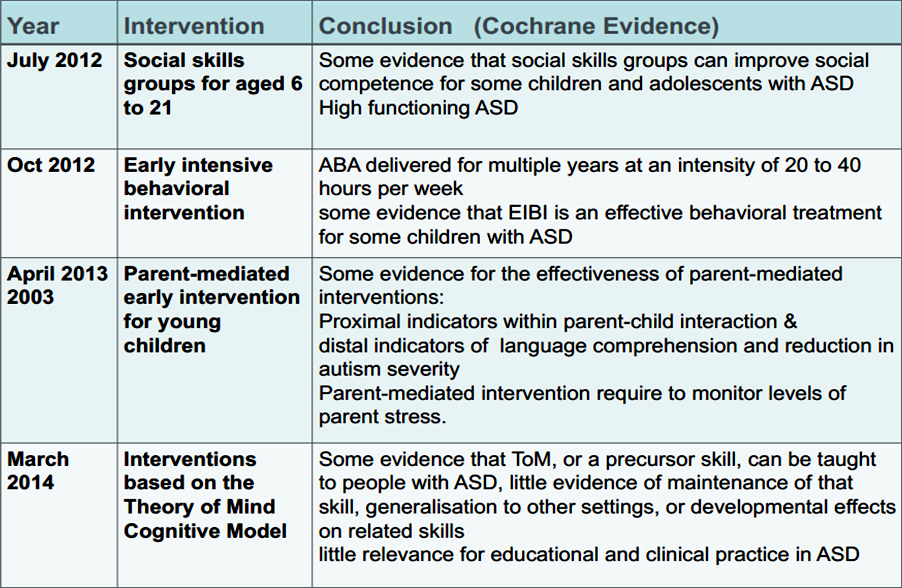
ABA: Evidence
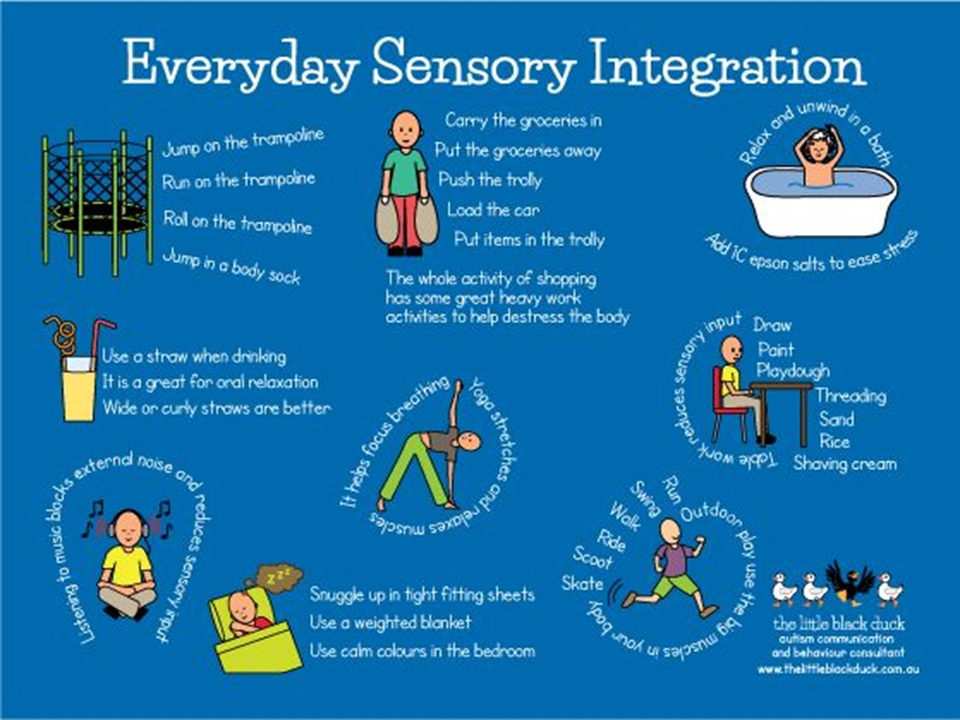
Sensory Integration Therapy
- Hypothesis: Impairment in sensory information processing in ASD
- Based on Ayres' Theory of sensory integration
- Play activities specifically designed to restore effective neurological processing by enhancing vestibular, proprioceptive and tactile systems
- Sensory diet: Specifically designed plan of biochemical and neurological inputs to promote and facilitate function

Sensory Diet
- Biochemical inputs:
- Sleep
- Nutrition
- Neurological inputs:
- Vestibular
- Proprioceptive
- Tactile
- Auditory
- Visual

Sensory Integration Therapy: Evidence
- 4 studies: Significant improvement in several autistic core symptoms
- Limitations
- Two studies used a standardized form of therapy
- Lack of standardized outcome measures
- Lack of well-defined control group
- Recommended by NICE guidelines, 2013
ASD: Medical Management
- Routine care: immunization, growth, nutrition, hygiene
- Psychopharmacology: core symptoms, associated symptoms and psychiatric illnesses
- Co morbidities: epilepsy, GI, behavior, psychiatric illnesses, sleep (identification & treatment)
Psychopharmacology
- Pharmacologic interventions may be considered for maladaptive behaviors such as aggression, self injurious behavior
- Repetitive behaviors (eg: perseveration, obsessions, compulsions, and stereotypic movements)
- Sleep disturbance, mood lability, irritability, anxiety, hyperactivity, inattention, destructive behavior, or other disruptive behaviors
- Repetitive behavior, obsessive-compulsive symptoms, stereotypic movement disorder: SSRIs (fluoxetine, fluvoxamine, citalopram), Atypical antipsychotic agents (risperidone, aripiprazole, olanzapine), Valproic acid
- ADHD: stimulants, atypical antipsychotic, clonidine
- Aggression, self injury: atypical antipsychotic, VPA, LEV, SSRIs
- Anxiety and depression: SSRIs
Pharmacologic Interventions: Evidence
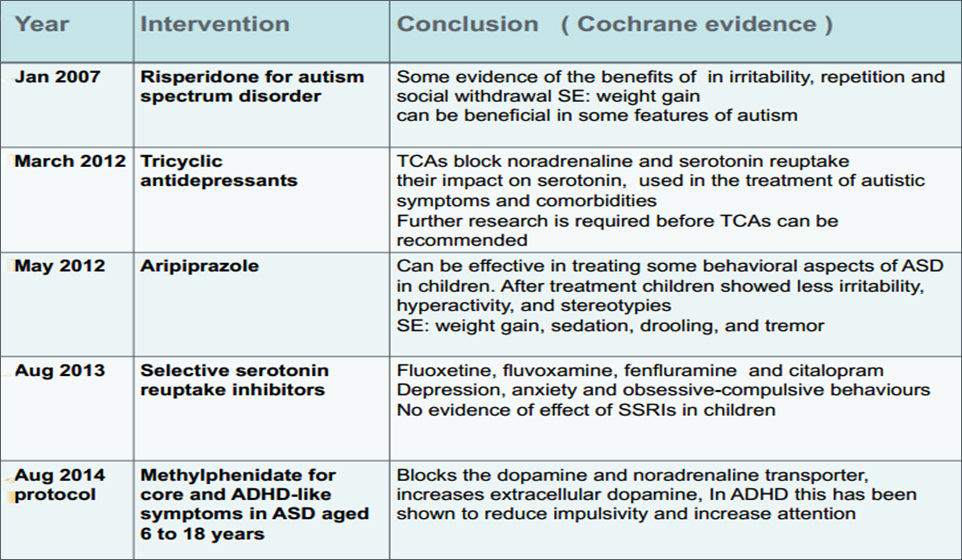
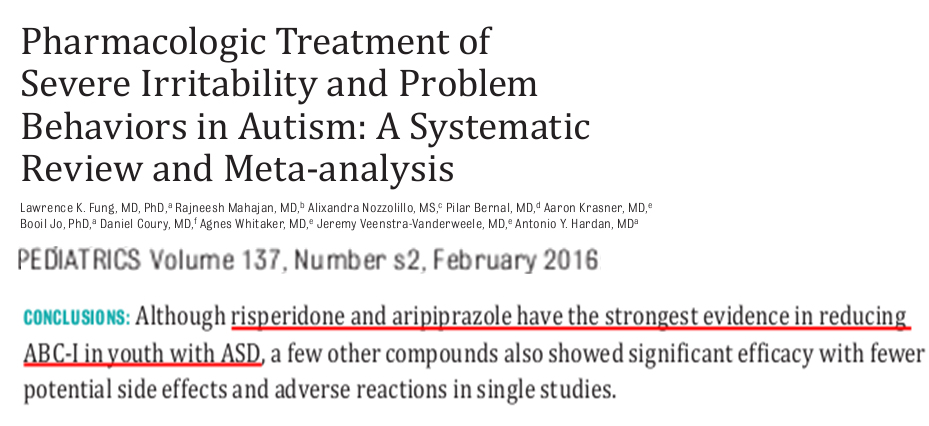
1 α2 adrenergic agonist (clonidine), 1 psychostimulant (methylphenidate), and 1 tricyclic antidepressant (tianeptine) demonstrated moderate effect sizes in decreasing ABC-I.
GI Disturbances
- Gastrointestinal symptoms (including abnormal stool pattern, frequent constipation, frequent vomiting, and frequent abdominal pain) reported in 70% of children with ASDs
- High rates of lymphoid nodular hyperplasia & histologically subtle esophagitis, gastritis, duodenitis, and colitis
- Routine specialized gastroenterological testing for asymptomatic children is not recommended
- Occult gastrointestinal discomfort should be considered in a child who presents with a change in behavior, such as outbursts of aggression or self-injury
- Effective management may provide global benefit
PEDIATRICS Volume120, Number5, November 2007
Sleep Disturbances 
- Estimated prevalence of 50% to 80%
- In a study at AIIMS, it was found that sleep problems affect upto 58 % of children with autism.
- Polysomnography studies show that children with ASD have altered sleep architecture includingshorter total sleep time and longer sleep latency than typically developing peers
Pediatrics. 2016;137(S2)
Sleep Disturbances: Melatonin
- Abnormality of melatonin regulation in children with ASDs
- Clinical studies have shown some benefit
- Small randomized, placebo-controlled trials showed increased sleep duration and reduced sleep latency
- Retrospective study of 107 children showed only 3 with side effects of daytime sleepiness and enuresis (Andersen, 2008)
- Recommendation: 1-3 mg 30 minutes prior to bedtime
EEG Abnormalities: Treat or Not
- Epileptiform abnormalities: 10% to 72% patients
- No well designed, controlled trials have defined a role for antiepileptic drug therapy for symptoms of ASD
- In absence of clinical epilepsy, treatment of epileptiform activity with AEDs has not been demonstrated to reverse the symptoms of ASD
Epilepsia, 48 (Suppl. 9):33–35, 2007
Management Guidelines for CSWS
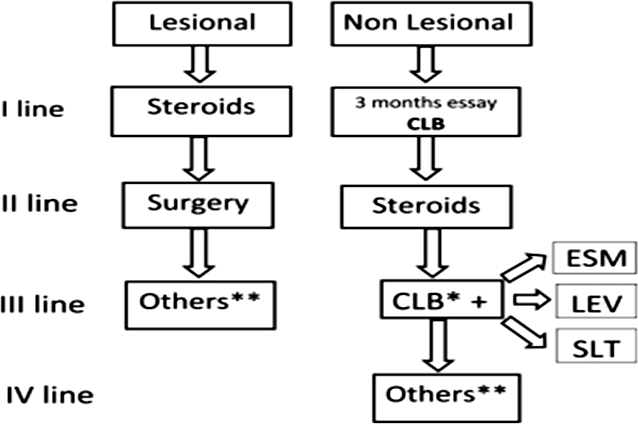
Veggiotti P et. al. Journal of Clinical Neurophysiology, February 2016
Anecdotal Therapies
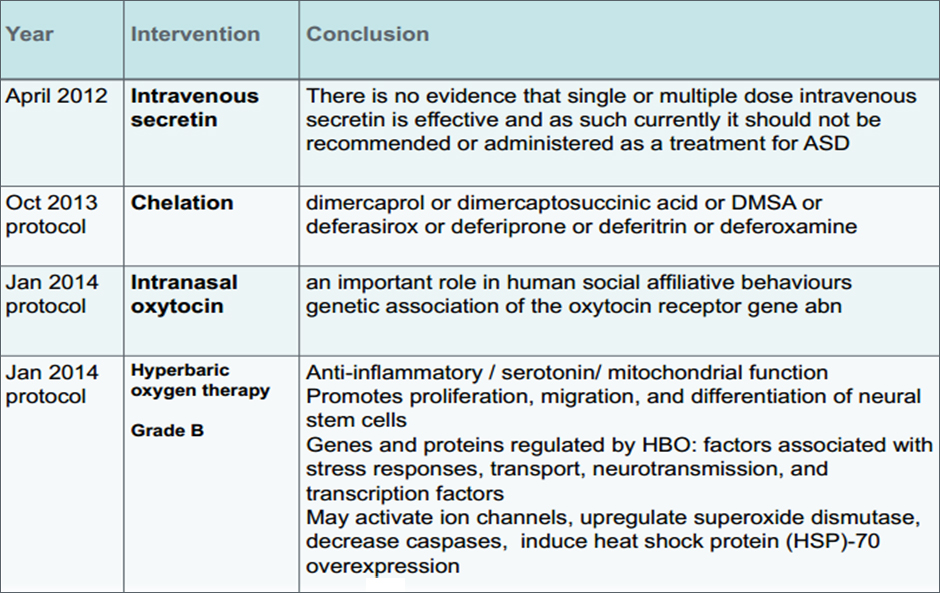
- IV Secretin
- Intranasal Oxytocin
- Chelation: DMSA and others
- HBOT
- Mesenchymal stem cell transplant (umb cord or peripheral), fetal stem cell
Anecdotal Therapies: Evidence
What is CAM?
- “A group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine”
- “A broad domain of healing resources that encompasses all health modalities, and practices other than those intrinsic to the politically dominant health systems of a particular society or culture in a given historical period”
- ASD: Vitamins, minerals, exclusion diets, yoga, music therapy………..
- Lack of “Gold Standard”
Who uses CAM?
- CAM perceived as “natural”, without side effects
- > 75% chose CAM based on perception of
safety, absence of side effects or prior
experience with side effects
- Internet and media
- Recommendations by friends or families
of other children with ASD
Hanson et al. Use of CAM among children diagnosed with ASD.
J Autism Dev Disord. 2007
Types of CAM
Biologically Based Treatments
- Dietary interventions
- Vitamin supplements
- Herbal remedies
- Chelation
- HBOT
Non Biologically Based Treatments
- Mind-body medicine (i.e., prayer, yoga, meditation, music, dance, and art)
- Manipulative and body-based practices (i.e., massage, chiropractic care, acupuncture, patterning)
How to Handle CAM?
- AAP Committee on Children with Disabilities
- CAM interventions should be discussed in a nonjudgmental manner
- Treating physician should provide “balanced advice about therapeutic options” and information about potential risks
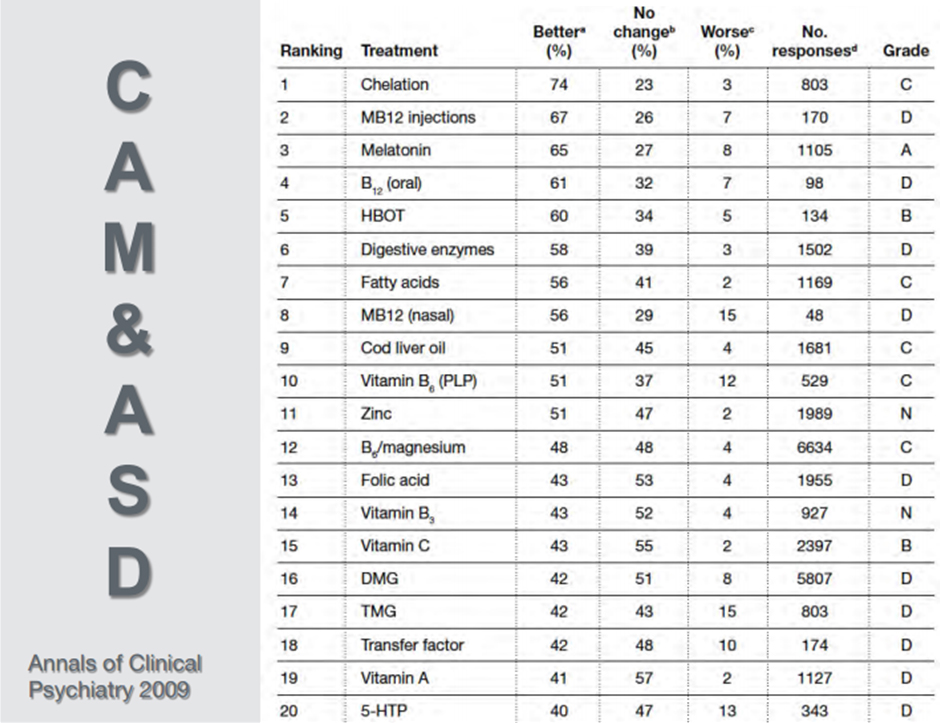
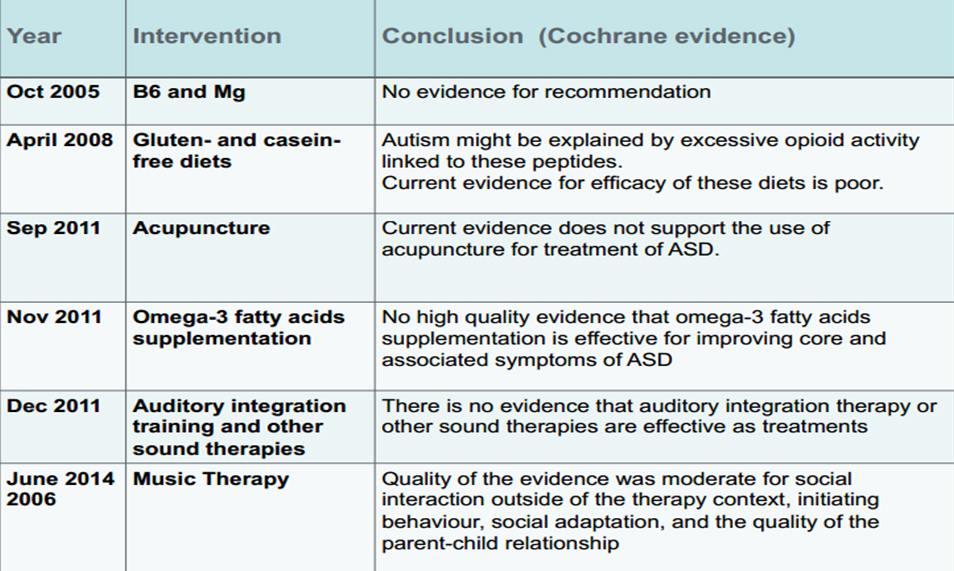
CAM: Evidence
CAMs that may be used
Recommendations: Sensory integration therapy
Experimental, Individual basis
- Pet therapy
- Drama therapy
- Music therapy
- Massage
- Yoga
Conclusion
- Educational intervention if initiated early and intensive, have shown some benefit
- Resperidone and Aripiprazole is recommended for Irritability and problem behaviors in ASD
- Melatonin is effective for sleep disturbances
- CAM should be looked at with open mind and weighed appropriately
Thank You