Long Face/ large ears/ large tested (postpubertally)
Angelman syndrome
Ataxic gait/ broad mouth/ persistent smile/ language delay/ seizures
CNS
Examine for tone/ reflexes/ neurological deficits
Children with ASD can have mild hypotonia
Focal neurologic findings, such as asymmetry in tone or reflexes, require further neurologic evaluation and possible neuroimaging
Filipek PA et al. J Autism Dev Disord 1999; 29;439
Ancillary Testing
To exclude conditions that may produce symptoms of ASD
To identify potentially treatable conditions associated with ASD
To define child's particular pattern of strength and weaknesses for education planning
Hearing assessment
Developmental/ intelligence testing with separate estimates for verbal/ non-verbal skills
Assessment of adaptive skills to document the presence of associated intellectual disability and to help establish priorities for treatment planning
Guided by history and examination to include EEG/ Genetic testing/ Neuroimaging
Diagnosis
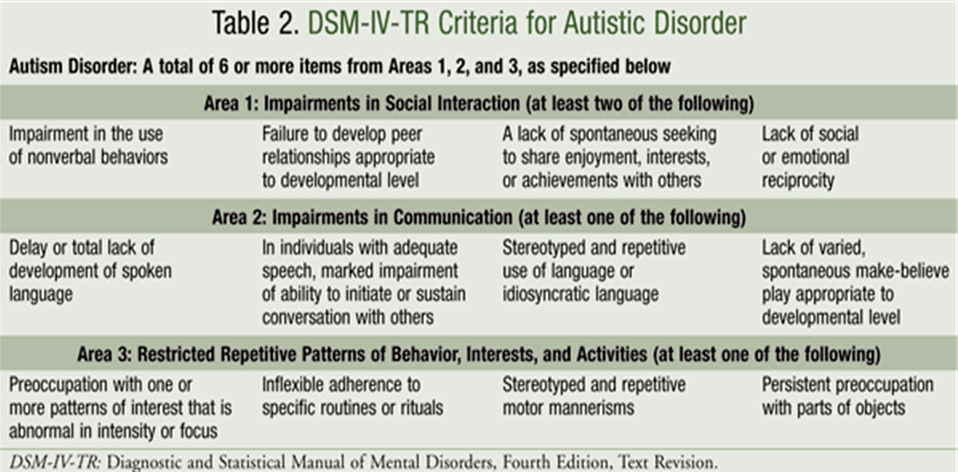
Diagnostic Criteria
DSM 5
Diagnostic Tools
INCLEN
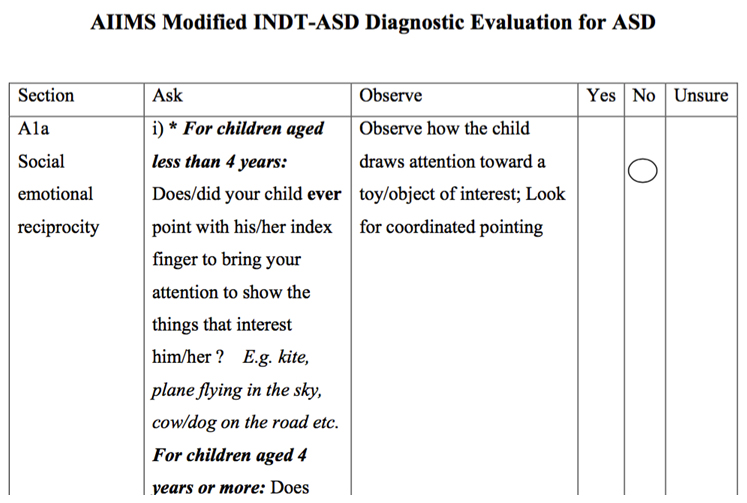
AIIMS Modified INDT-ASD Tool
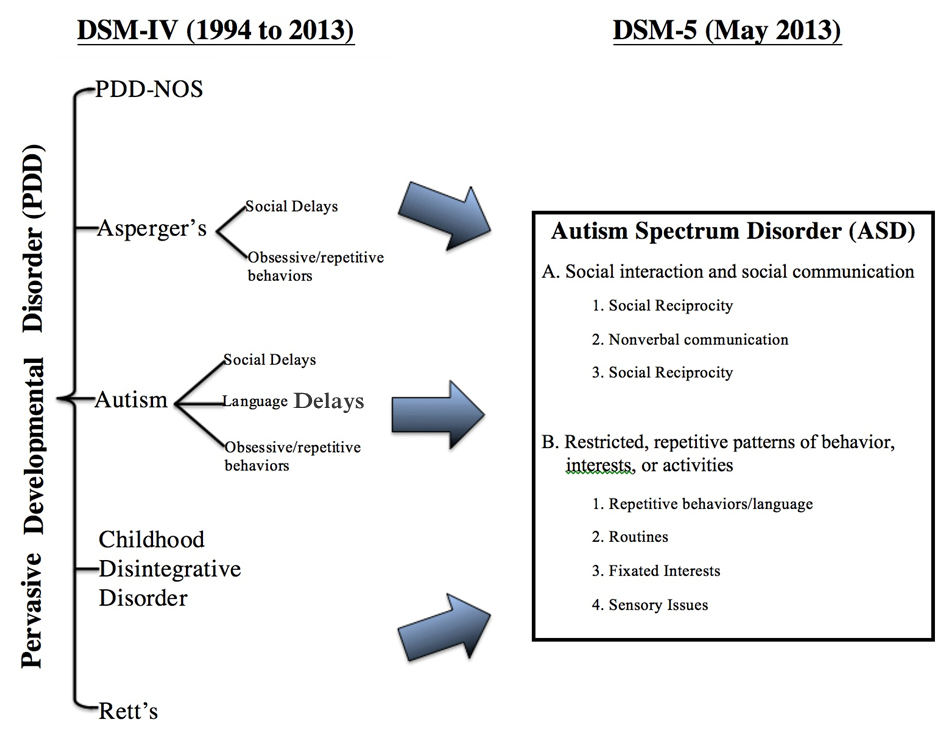
DSM-IV
DSM-5
DSM 5 (2013)
A single diagnosis replaces the sub-divisions
Diagnosis based on 2 areas
Deficits in social communication and Fixated interests
Repetitive behavior
Restriction of onset age loosened from 3years to “early developmental period”
New severity ranking
Diagnostic Criteria: DSM 5
According to the DSM-5 criteria, a diagnosis of ASD requires all of the following
Persistent deficits in social communication and social interaction in multiple settings; demonstrated by deficits in all three of the following (either currently or by history):
Social-emotional reciprocity (eg, failure of back-and-forth conversation; reduced sharing of interests, emotions)
Social-emotional reciprocity (e.g., failure of back-and-forth conversation; reduced sharing of interests, emotions)
Nonverbal communicative behaviors used for social interaction (e.g., poorly integrated verbal and nonverbal communication; abnormal eye contact or body language; poor understanding of gestures)
Developing, maintaining, and understanding relationships (e.g., difficulty adjusting behavior to social setting; difficulty making friends; lack of interest in peers)
Restricted, repetitive patterns of behavior, interests, or activities; demonstrated by ≥2 of the following (either currently or by history)
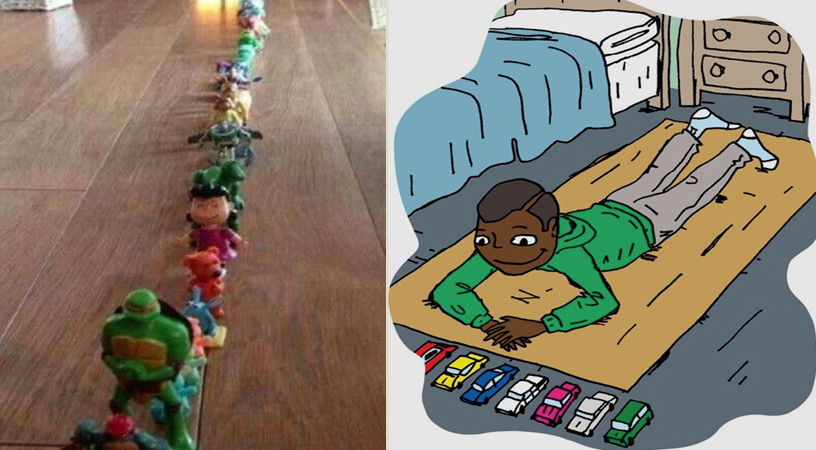
Stereotyped or repetitive movements, use of objects, or speech (e.g., stereotypes, echolalia, ordering toys, etc)
Insistence on sameness, unwavering adherence to routines, or ritualized patterns of behavior (verbal or nonverbal)
Highly restricted, fixated interests that are abnormal in strength or focus (e.g., preoccupation with certain objects; perseverative interests)
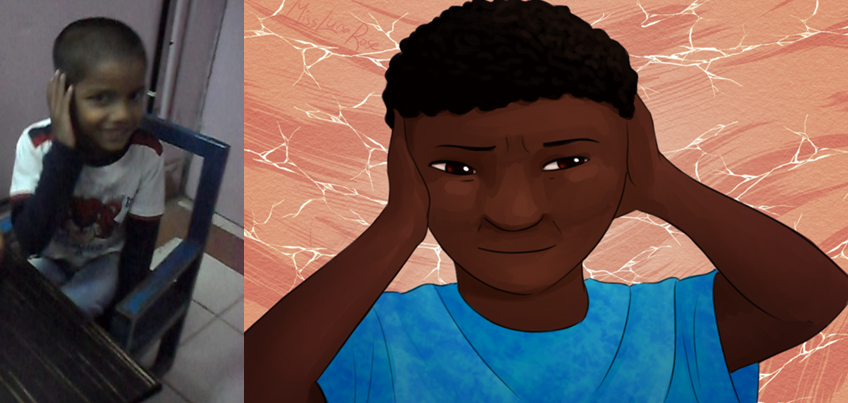
Increased or decreased response to sensory input or unusual interest in sensory aspects of the environment (e.g., adverse response to particular sounds; apparent indifference to temperature; excessive touching/smelling of objects)
The symptoms must impair function (e.g., social, academic)
The symptoms must be present in the early developmental period. However, they may become apparent only after social demands exceed limited capacity; in later life, symptoms may be masked by learned strategies
The symptoms are not better explained by intellectual disability or global developmental delay
American Psychiatric Association. Autism spectrum disorder. In: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, American Psychiatric Association, Arlington, VA 2013. p.50
Diagnostic Criteria: DSM 5
Severity Level
Social communication/interaction
Level 1 ("Requiring support") – Noticeable impairment without support; difficulty initiating social interactions, atypical or unsuccessful responses to social overtures; decreased interest in social interactions; failure of back and forth conversation; attempts to make friends odd and unsuccessful
Level 2 ("Requiring substantial support") – Marked deficits in communication; impairments apparent even with supports; limited initiation of social interactions; reduced/abnormal response to social overtures
Level 3 ("Requiring very substantial support") – Severe impairments in functioning; very limited initiation of social interactions; minimal response to social overtures from others
Repetitive/Restricted Behavior
Level 1 ("Requiring support") – Behaviors significantly interfere with function; difficulty switching between activities; independence limited by problems with organization and planning
Level 2 ("Requiring substantial support") – Behaviors sufficiently frequent to be obvious to casual observer; behaviors interfere with function in a variety of settings; distress and/or difficulty changing focus or action
Level 3 ("Requiring very substantial support") – Behaviors markedly interfere with function in all spheres; extreme difficulty coping with change; great distress/difficulty changing focus or action
American Psychiatric Association. Autism spectrum disorder. In: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, American Psychiatric Association, Arlington, VA 2013. p.50
Diagnostic Criteria: DSM 5
Other Specifiers
Clinicians specify the presence or absence of the following accompanying or associated conditions
Intellectual impairment; to diagnose comorbid ASD and intellectual disability, social communication should be below that expected for general developmental level
Language impairment (eg, nonverbal, single words only, etc)
Known medical or genetic condition (eg, epilepsy, Rett syndrome, Down syndrome, etc) or environmental factor (eg, valproate, fetal alcohol exposure)
Another neurodevelopmental, mental, or behavioral disorder (eg, attention deficit hyperactivity disorder, developmental coordination disorder, etc)
Catatonia
American Psychiatric Association. Autism spectrum disorder. In: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, American Psychiatric Association, Arlington, VA 2013. p.50
Diagnostic Tools
Tools based on the diagnostic criteria
Questions adapted to suit the cultural setting/ abolish language barriers
Neuro-developmental Disabilities Among Children in India: An INCLEN Study
Juneja M, Mishra D, Russell PSS, Gulati S, Deshmukh V, Tudu P, et al. INCLEN Diagnostic Tool for Autism Spectrum Disorder (INDT-ASD): development and validation. Indian Pediatr. 2014 May;51(5):359–65
Other Tools
Autism Behavior Checklist
List of 57 questions to be completed by a parent or teacher
The questions are divided into five categories: sensory, relating, body and object use, language, and social and self-help
Designed primarily to identify children with autism from a population of school-age children with severe disabilities
However, it has been used with children as young as three years
The reported sensitivity and specificity of the ABC in referral samples range from 38 to 58 percent and 76 to 97 percent, respectively
Johnson CP et al. Pediatrics 2007; 120:1183
Krug DA et al. J Child Psychol Psychiatry 1980; 21:221
Childhood Autism Rating Scale, Second Edition (CARS-2)
15-item direct-observation instrument designed to facilitate the diagnosis of autism in children two years of age and older
Each of the items is scored on a four-point rating scale
CARS-2 is well correlated with the DSM-IV criteria and discriminates ASD from other developmental disorders better than the ABC
CARS-2 is intended for use by a trained clinician and takes approximately 20 to 30 minutes to administer
In a systematic review, the average sensitivity and specificity were 82 and 80 percent, respectively, for ASD
Filipek PA et al. J Autism Dev Disord 1999; 29:439
Rellini E et al. J Autism Dev Disord 2004; 34:703
Gilliam Autism Rating Scale
Consists of a checklist of 56 items for parents based on DSM diagnostic criteria
Autism Diagnostic Interview-Revised (ADI-R)
2 to 3 hour clinical interview that probes for autistic symptoms
Autism Diagnostic Observation Schedule (ADOS)
Available for use in individuals age 12 months through adulthood
Conclusion
Diagnosis requires comprehensive evaluation preferably a team
Diagnosis is established based on DSM-5 Criteria
Evaluation uses tools that facilitate application of DSM-5 and establishment of diagnosis
Assessment should be made for primary concerns so that they can be addressed specifically